Mental health services, individuals and the ‘social body’ at the time of the coronavirus
Roberto Mezzina, ex-Director of the WHO Collaborating Center, DSM of Trieste
"The coronavirus emergency has necessarily put everything else in the background, conditioning and changing our lives.... There has never been a need for mental health policies as here is now, precisely because the whole Italian population, and sooner or later the globe, will suffer from a formidable discomfort, which touches and will touch everyone, an not only those who already have diagnosed psychiatric disorders, upsetting the world as we have known it."
Mental health services, individuals and the ‘social body’ at the time of the coronavirus
Roberto Mezzina, ex-Director of the WHO Collaborating Center, DSM of Trieste.
The coronavirus emergency has necessarily put everything else in the background, conditioning and changing our lives. If healthcare in Italy is subjected to a great deal of distress, to an unprecedented challenge, mental healthcare, daughter of a minor god, suffers in silence. The impoverishment of services, their reduction and merger, the shortage of staff, already reported for many years so far, adds to the fact of being placed today at the bottom of the list of health priorities. The level of the threat, as in war, appears higher, and the expression "protection of mental health" sounds almost pleonastic in many health contexts. Yet, in the era in which nobody can question the lawfulness of a “bio-politics" dictated by medicine, there has never been a need for mental health policies as now, precisely because the whole Italian population, and sooner or later of the globe, suffers from a formidable discomfort, which touches and will touch everyone, and not only those who already have diagnosed psychiatric disorders, upsetting the world as we have known it.
There is a risk of the final, legitimised and even understandable, catastrophe of the Italian mental health system. It is news of these days of some Diagnosis and Treatment Services in Lombardy that are being converted back to Covid-19 departments, with all the staff (although absolutely and obviously not prepared for the new tasks assigned). Many other services are closed, or severely limited, and limited basic care - such as all "specialist" outpatient care - is strictly necessary and by appointment; which is exactly the opposite of flexible service for a distressed population. What is a priority is difficult to identify. Therefore, in these hours, guidelines and recommendations are being developed to guide healthcare companies, departments and operators on what to do.
It appears evident that the "social body", to which Basaglia constantly referred, seems to withdraw. That COVID 19 seems at the outset a war made of isolated individuals, of loneliness. But it is also of families; or small local communities, such as the condominium, the neighbourhood; and virtual networks, small and open, or global. But inevitably it touches the whole "social body". Inside, the mental health worker is one of many. He does not have to cure Covid syndrome, but nevertheless he must continue to work, because there is a need for many levels of support, including psychological and psychiatric. And there is no real distinction between who cares and who is cared for, paradoxically the operator can transmit the disease, also because adequate precautions are not possible. It is useless to underline the well-known situation in which elementary medical-surgical devices, masks and disinfectants are almost totally missing.
So on the one hand the uselessness and even the harmfulness of an outpatient setting such as that which was held so far in the services, often with crowded waiting rooms, and of the same hospitalisations, if not strictly necessary, are clear: all imply a potential risk of the "organic body" of each. However, the "different" services, those born from the 1978 reform law, suffer the most. It was said to abolish the distance with the patient, not to "keep us at a distance". The relationship, the main instrument of therapy and also of assistance in mental health, cannot be used freely and directly. The group, the collective, are necessarily constrained and finally abolished; even touching the body, which is the medium, individual and social at the same time, where anguish is released, is inhibited: the "organic body" is now a potential source of danger.
The services of personal support, home and educational assistance, offered above all by social cooperatives and no profit sector, slow down or stop in the absence of adequate prevention tools.
The social, therapeutic and rehabilitative values of attending a Mental Health Center or a Day Center are in crisis and largely fail. Everywhere there is a restrained, guarded sociality.
Here is revealed all the fragility of a mental health made of “places”. Paradoxically, it is precisely the extra-hospital environments, those of normality, of the community, of common life, that suffer the most because they can be transformed into places of infection by being places of meeting and exchange. This range includes all the communities where temporary or longer-term forms of coexistence take place, especially with a 24-hour residence, where epidemic outbreaks involving operators and guests have already occurred, as in rest homes.
In spite of everything, never as now is it necessary to gather around services such as anchors for the protection of mental health. Services should be urgently saved, while rethinking mental health in the coronavirus era. That will last at least for a while, we know, and in any case it is already transforming individual and collective behaviors and habits.
If the sociality, in a logic of "restitution to the social body", was the utopia of Basaglia and of the reform, what to do now that the social networks shrink to the essential, while all the communication media expand, and especially the social media? You live connected through the internet, or on the phone, or attached to the TV. While you need to be informed, too much exposure, and especially exposure to unreliable sources, can increase stress.
Studies on individual behaviours don't give much help, they don't make much sense. They mainly use and emphasise this notion of stress and the consequent post-traumatic-stress-disorder (the famous PTSD). The timely publication in Lancet Psychiatry of a review on the psychological effects of the quarantine, based on other epidemics, from SARS onwards, is these days. But here it is not about quarantining individuals affected, or positive for infection, as potential sources of contagion. The "lockdown", being locked in the house, which Italy and now other countries are experiencing and living, is a huge collective experiment, a new “Norm”: a generalised condition that affects everyone, especially those who are really at home and do not go to your workplace, health care facilities, industrial production or essential services every day.
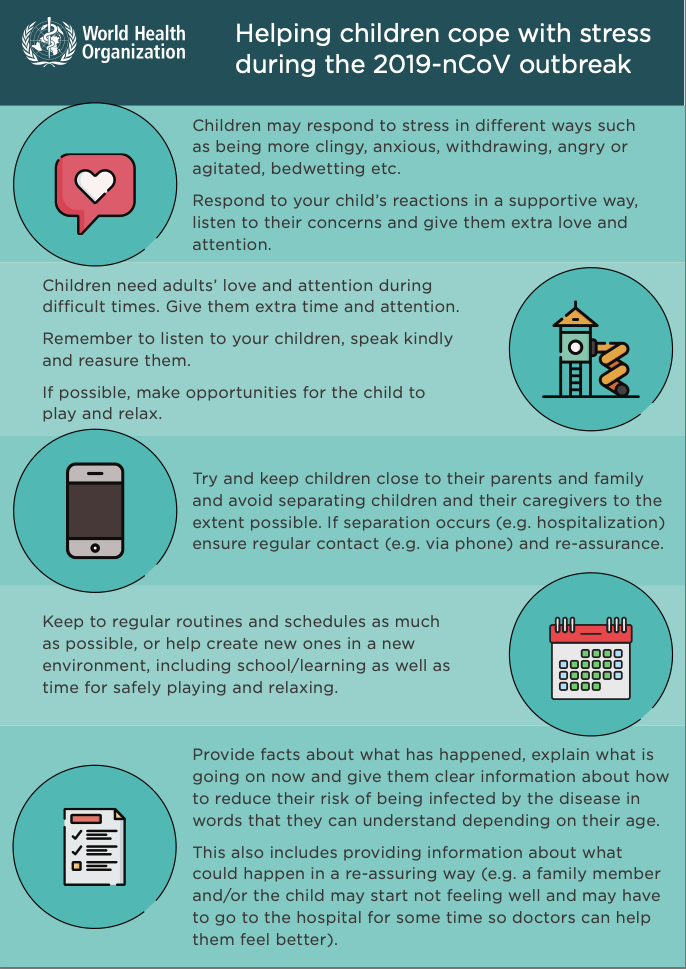
Starting from the Lancet review, the American Psychiatric Association through the University of Bethesda, and now the Canadian, have made recommendations. Mental Health Europe has released a simple list of tips. WHO has made a poster on the different forms of help between people, with attention to children, even an invitation to alternative forms of greeting to avoid handshakes or hugs. The IASC has updated its guidelines for humanitarian emergency intervention in the population exposed to Covid, but it is already old because it does not contemplate the total closure of a country, or of several countries. Many recommendations concern the same health workers and among them those of mental health, who must take care of their patients but also that of their mental well-being during the quarantine periods, and at work, which must continue. They must be able to eat, drink and sleep regularly, take breaks, communicate with colleagues and loved ones also through the media, and ensure that both their family and organisation are safe and have established a plan in case of contagion.
We must think quickly about how and what to communicate, do and say in Italy, to help citizens' mental health, from the weakest to the most guaranteed. Studies confirm - but how could this not be the case - that in situations similar to that of the "lockdown" increase boredom, frustration, and even the level of anxiety, which dilates the fear of infection up to panic, and cenestopathies, but not too much. We all equip ourselves in the face of a danger, which is strong and present, although invisible. Few implement denial and escape from reality, with obstinacy in maintaining their lifestyle "despite everything". But above all with isolation you can experience a condition of generalised trauma, with potential short and long-term post-traumatic effects.
Meanwhile, the ancient social reception of the disease as guilt, individual and collective, something that psychiatry has known in history and still today permeates popular culture, above all where the medical model has not replaced the old beliefs and covered every objection. We have already seen unjustified forms of prejudice and stigma triggered against individuals (ex-sick) or entire populations or ethnic groups.
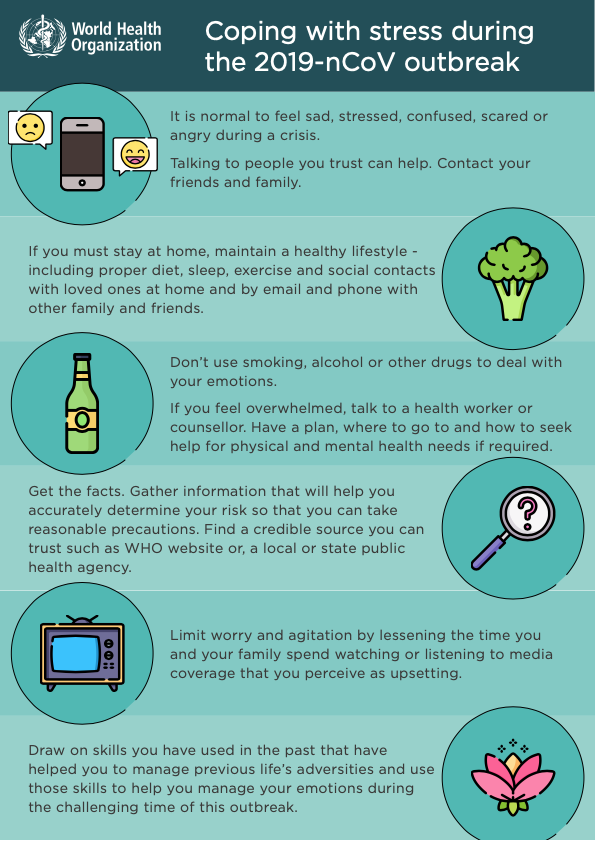
It is therefore urgent to give and find meaning in the quarantine, beyond the right rules of hygiene that impose it. Many documents contain simple advice for those who are in various forms of quarantine, such as those now generalised to all and which even spontaneously everyone tries to implement. In addition to maintaining a restful sleep and eating regular meals, exercise (at home!); limit the use of alcohol, tobacco and other drugs; talk to loved ones, even about worries and fears; practice any relaxation strategies, engage in hobbies and pleasant activities. There are tips for those with children, or older people, and for families as such.
It's not that easy. Social detachment also hangs over those who cannot, or do not know (and sometimes do not want to) defend themselves. If, on the one hand, people with more serious mental problems, as it is recognised, prove capable of coping and also of helping in emergency conditions - as happens, for example, in wars - on the other, the social isolation of those who have psychotic problems is now ironically allowed and "normalised" as behaviour imposed on everyone. But many have disappeared from the services, holed up in the house again. Families, where there are, keep or recover the sick: ties are strengthened in times of danger. But both the alienation determined by the absence of social ties of the former, and the conflicts in the latter, can sharpen suddenly and lead to moments of crisis that must be absolutely prevented.
In the general population, in an approved situation in which moving, exercising together, eating or drinking in a group, conviviality, even singing or playing together are inhibited, it is necessary to stay side by side in the everyday life, in an intimacy or forced promiscuity, which is that of the family (for those who have it). Others are forced to choose whether to be alone or to live together if they have a relationship. Who has a garden, a second home, a place of retreat and escape, is lucky.
In this predominantly domestic scene, can services appear with caution? A series of people then, the most fragile - and here not only in the medical or psychiatric sense, but socially - must be reached at home, either by telephone (having a landline or a mobile phone is now recognised as a necessity also for health, i.e. electronics stores are allowed to stay open) which, where physically necessary, to offer support in person as well as drugs. This with due caution, and in a very consensual situation, and of conscious, bilateral, maximum containment of risk. The outpatient model does not foresee it, that is already a first challenge. We need to prioritise services, identify who needs them most. It's called selective prevention. Higher-risk psychopathological profiles are suggested (patients with delusions, obsessive-compulsive thoughts and behaviours, somatic symptoms, or previously exposed to severe trauma) for whom more frequent contacts can help respond to emerging concerns, which can help avoid serious exacerbations or hospitalisations. But most of all, individual stories and situations need to be kept in mind. It is also necessary to invent forms of teleworking, telemedicine or tele-psychiatry, and which are not cold but affective, a sort of remote “tele-heart”.
The social gradient of mental health is confirmed in all its relevance and drama: the discomfort of the poorest, of those who are alone, or even amassed, in tight holes. Many may not have food and may not access social canteens or meals provided in the services themselves. Remember to ensure basic needs, even with meal deliveries. The homeless, then, are lost in a social nothingness, without alms, not even because there are no people on the streets, without hot food if not with praiseworthy efforts of part of the volunteer sector. Here the services must "outreach", reach those who do not access them, even on the street, and powerfully support those who guarantee survival, mobilizsng all the possible resources of communities, neighbourhoods, associations, churches.
More information and reassurance should be provided; but above all it is necessary to give meaning to isolation. This applies to all of us, to all of society and is an extraordinary element of universal prevention, that is addressed to the whole population. Here emerges the need to get out of individualistic visions and opt without delay for sharing and solidarity, civil and social. Now it is necessary to raise the sense of being part of a community, and services can and must act as bridges.
It will then be necessary to valorise and study individual and collective resilience factors, and coping strategies for a "recovery" that will never be an interpersonal and social fact as ever. We already talk about the "Whole of Society approach", a global collective approach (IASC).
The new forms of social connection that are developing in this collective long-endurance effort will have to be enhanced. As well as a rediscovery of the self, and a training that is not just physical – e.g. fitness, the healthy lifestyle that is also in fashion - but a Foucaultian "self-care". What do we really need? What is essential? While we are thrown back into ourselves, in something unheard of for all of us, listening to ourselves and focusing on our body, even on our breath, is opposed to it and perhaps the sense of a community, of a common struggle prevails. The sense of a collective heroism, where the fragmented and mediated social body reconnects ideally, or perhaps even concretely, in multiple forms of help and survival. And this is the mental health of an entire society. So we defend the services, which interpret and mediate this “social body”, while defending ourselves.
References
Basaglia F. Madness / Delirium. In Hughes NS, Lowell A (eds), Psychiatry inside out. Selected writings of Franco Basaglia. New York: Columbia University Press: New York, 1987: 231-263.
Manderscheid RW. Preparing for Pandemic Avian Influenza: Ensuring Mental Health Services and Mitigating Panic. Archives of Psychiatric Nursing, Vol. 21, No. 1 (February), 2007: 64–67
Brooks SK, Webster RK, Smith LE, Woodland L, Wessely S, Greenberg N, Rubin GJ. The psychological impact of quarantine and how to reduce it: rapid review of the evidence. Lancet 2020; 395: 912–20. Published Online February 26, 2020.
United Nations Inter Agency Standing Committee (IASC). Psychosocial Support in Emergency Setting. Briefing note on addressing mental health and psychosocial aspects of COVID-19 Outbreak - Version 1.0, February 2020
McGushin, E. Foucault's theory and practice of subjectivity. In Taylor, D. (red.) Michel Foucault: Key Concepts, 127-142. Acumen Publishing Ltd., 2011. ISBN 978-1-84465-234-1
American Psychiatric Association (APA). COVID-19 Mental Health Impacts: Resources for Psychiatrists. Published Online, Mar 12, 2020.
Resources
Here are some resources we have found that could be helpful if you are concerned about the consequences of the Corona Virus pandemic for your mental health and also for the delivery of mental health support over this period.
Here are the main points for all of us:
- Limit the news and be careful what you read
- Have breaks from social media and mute things which are triggering
- Try to avoid speculation and look up reputable sources on the outbreak
- Wash your hands - but not excessively
- Stay connected with people
- Talk to your children
- Avoid burnout
- Try not to make assumptions
- Try to anticipate distress
Some points for mental health workers:
- 'Facts minimize fear.' Stay informed from trusted sources.
- 'You must always return to yourself."
- 'Think about mental health as part of the public health response.'
- 'Social isolation is associated with poor mental health.'
- 'Shift narratives away from number of deaths toward number of recoveries.'
- Above all, the common thread among all these experts was that we need to stay informed by trusted sources.
Briefings and Notices
Briefing Note about MHPSS aspects of COVID-19
With inputs from all its member organizations, the IASC MHPSS RG recently finalized a Briefing Note about MHPSS aspects of the 2019 novel coronavirus (COVID-19) outbreak.
This document summarizes key mental health and psychosocial support (MHPSS) considerations in relation to the COVID-19 outbreak, such as appropriate MHPSS responses, overarching principles and globally recommended activities. More specifically, it contains useful guidance about how to, during the COVID-19 outbreak:
- help older adults cope with stress,
- support the needs of people with disabilities,
- design messages & activities to help children deal with stress,
- set up MHPSS activities for adults in isolation/quarantine,
- provide support to response workers, and
- circulate community MHPSS messages.
It also contains numerous references and information sources. It is available in English, Chinese (traditional + simplified), and Arabic.
Go here
Mental Health and Psychosocial Considerations During COVID-19 Outbreak
These mental health considerations were developed by the WHO’s Department of Mental Health and Substance Use asmessages targeting different groups to support for mental and psychosocial well-being during COVID-19 outbreak.
Go here
Articles:
Coronavirus: How to protect your mental health BBC News, 16th March 2020. Click on title for full article.
How to look after your mental health during the Coronavirus outbreak from the Mental Health Foundation.
Managing mental health during coronavirus - experts around the world share insights from the World Economic Forum